


{kind=link}
- Lyme neuroborreliosis creates white matter lesions on brain MRI that are nearly identical to MS plaques. Radiologists with decades of experience can’t reliably tell them apart on imaging alone.
- About 14% of patients later confirmed to have Lyme disease were initially told they had MS. That’s roughly one in seven people starting the wrong treatment.
- The standard Lyme blood test – the two-tier ELISA plus Western blot – has documented sensitivity gaps for late-stage neurological Lyme. One negative blood draw does not close the book.
- A spinal tap is one of the strongest tools for separating the two. Oligoclonal bands show up in 85-90% of true MS cases. When they’re absent, other explanations deserve serious attention.
- MS treatment suppresses your immune system. Lyme treatment is antibiotics. These are opposite approaches, and being on the wrong one doesn’t just fail to help – it makes things actively worse.
- Every new MS diagnosis deserves a proper Lyme evaluation before disease-modifying therapy starts. Especially if you’ve spent any time outdoors in tick-endemic regions.
A Closer Look at This Brain MRI
Those red arrows are pointing at hyperintense white matter lesions – bright white spots that appear on a type of MRI sequence called T2-weighted or FLAIR imaging. In plain terms, those bright areas represent tissue that’s inflamed, damaged, or both. Something is attacking the myelin – the insulating layer wrapped around nerve fibers in the brain – and leaving visible marks behind.
Now here’s what you need to understand about this scan. The lesions are scattered across both hemispheres of the brain. Some are sitting in the subcortical white matter, closer to the surface. Others appear deeper, near the periventricular regions around the brain’s central fluid-filled spaces. They’re the right size and shape to satisfy the imaging criteria most neurologists use for an MS diagnosis.
If you brought this exact MRI into ten neurology offices, most of them would start an MS conversation. The pattern fits. The boxes get checked.
But the caption on that image - "Lyme can cause brain lesions that are often confused with multiple sclerosis" - is not exaggerating. The bacterium Borrelia burgdorferi, when it gets into the central nervous system, triggers an inflammatory response that damages myelin and leaves lesions on MRI that are radiologically indistinguishable from MS plaques in a significant number of cases.
Same bright spots. Same locations. Same sizes. Different disease entirely.
That scan cannot tell you which one it is. And that single fact is the reason this article exists.
How a Lyme Patient Ends Up With an MS Diagnosis
More easily than anyone wants to admit.
You walk into a neurology clinic. You’re exhausted – not regular tired, but the kind of fatigue where your bones feel heavy and sleep doesn’t touch it. Your fingers have been going numb for weeks. You keep losing words mid-sentence, and it’s scaring you. Maybe your vision went funny for a few days. Maybe you tripped going up the stairs because your legs didn’t cooperate.
Your neurologist listens, nods, orders a brain MRI. The images come back covered in white matter lesions, looking a lot like the scan above. The diagnosis follows quickly. MS.
And most of the time, that call is right. MS is common in neurological practice. The pattern recognition kicks in fast because neurologists see this presentation constantly.
But about 14% of the time, the patient actually has Lyme disease. One in seven. Those are real people who walked out of that appointment with the wrong label, started immunosuppressive medications they didn't need, and left a treatable bacterial infection to keep grinding through their nervous system unchecked.
The symptom overlap between these two conditions is wide enough to fool even careful doctors:
- Crushing fatigue that doesn’t improve with rest.
- Numbness and tingling in the hands, feet, arms, or legs.
- Cognitive fog – losing words, forgetting things you just heard, struggling to concentrate.
- Vision changes including inflammation of the optic nerve.
- Muscle weakness that comes and goes unpredictably.
- Balance and coordination problems affecting walking and fine motor tasks.
- Bladder urgency and frequency.
A patient walks in with half that list and a brain MRI full of white spots, and I get why MS comes to mind first. But “first” shouldn’t mean “only.”
What Should Actually Separate These Two Diagnoses
The differences are there. They just don’t wave a flag at you from across the room. You have to go looking, and that means spending more time than a single office visit allows.
The Lesion Pattern on Your MRI
Go back to that scan image for a second. Look at where those spots are sitting.
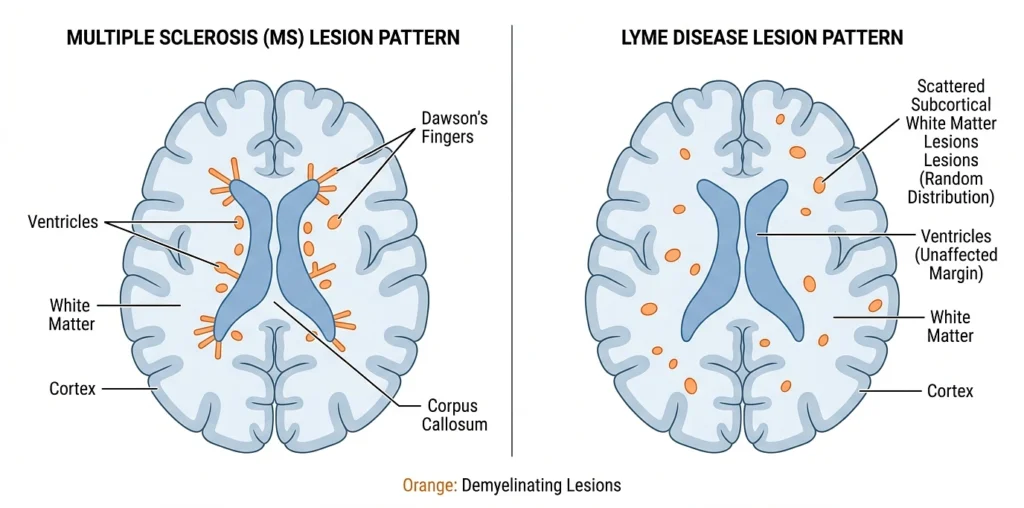
MS has a characteristic pattern. The lesions tend to cluster around the ventricles – the fluid-filled cavities deep in the center of the brain. They often stretch outward from the ventricles in elongated shapes perpendicular to the ventricular walls. Neurologists call these Dawson’s fingers, and they’re fairly specific to MS because they follow the path of small veins that drain the periventricular white matter. When a scan shows that pattern, MS moves to the top of the list.
Lyme lesions behave differently. They tend to scatter through the subcortical white matter more randomly, without the neat periventricular organization or the finger-like projections. Just spots, spread around, without an obvious anatomical logic behind their placement.
This isn’t foolproof – nothing in medicine is. Some Lyme patients get periventricular lesions. Some MS patients have more scattered patterns. But when a radiology report describes subcortical lesions without mentioning Dawson’s fingers or periventricular predominance, that should trigger a question in someone’s mind. What else could explain this?
The Lumbar Puncture – This Is Where You Get Real Answers
If I had to pick one test to separate MS from Lyme neuroborreliosis, it would be the spinal tap. No contest.
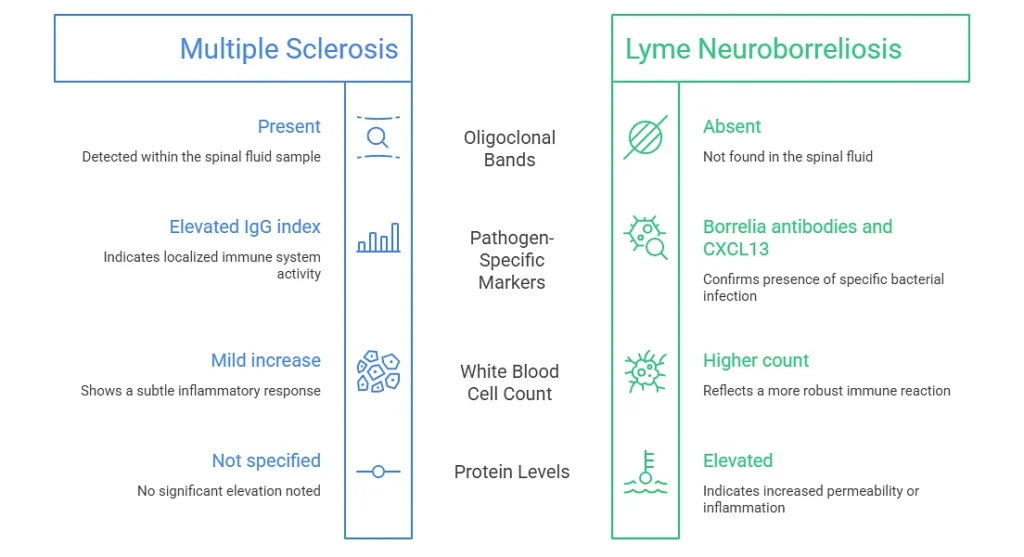
What MS looks like in spinal fluid:
- Oligoclonal bands – specific immunoglobulin patterns found in the cerebrospinal fluid but not in the blood. Present in roughly 85-90% of confirmed MS cases. This is one of the strongest laboratory markers for the disease.
- Elevated IgG index – a sign of increased antibody production inside the central nervous system.
- Mild lymphocytic pleocytosis – a modest bump in white blood cell count, though this varies.
What Lyme neuroborreliosis looks like in spinal fluid:
- Oligoclonal bands usually absent or showing a different pattern than what MS typically produces.
- More pronounced lymphocytic pleocytosis – a higher white blood cell count than you’d expect with MS.
- Elevated protein levels in the CSF.
- Intrathecal Borrelia-specific antibody production – the nervous system is making its own antibodies against the Lyme bacteria. Tested by comparing Lyme antibody ratios in spinal fluid versus blood. A high CSF-to-serum ratio is strong evidence for active neuroborreliosis.
- Elevated CXCL13 chemokine – this marker spikes during active neuroborreliosis and drops once antibiotic treatment starts. European clinics have been using it for years and it’s gaining ground in US practice.
Here’s the takeaway I want you to hold onto: if your lumbar puncture came back without oligoclonal bands, that finding alone should pump the brakes on an MS diagnosis. It doesn’t rule MS out completely – there’s still that 10-15% of MS patients who don’t have them – but it absolutely should expand the conversation to include other possibilities. Lyme being chief among them.
History Clues Your Neurologist Might Not Have Asked About
This part bothers me more than anything else in this whole discussion. By the time a patient is sitting in a neurology office with MRI images on the screen, everyone is zoomed in on the brain and the neuro symptoms. Nobody’s reaching back three months, six months, a year, to ask about things that happened before the numbness started.
But those earlier symptoms can crack the case wide open.
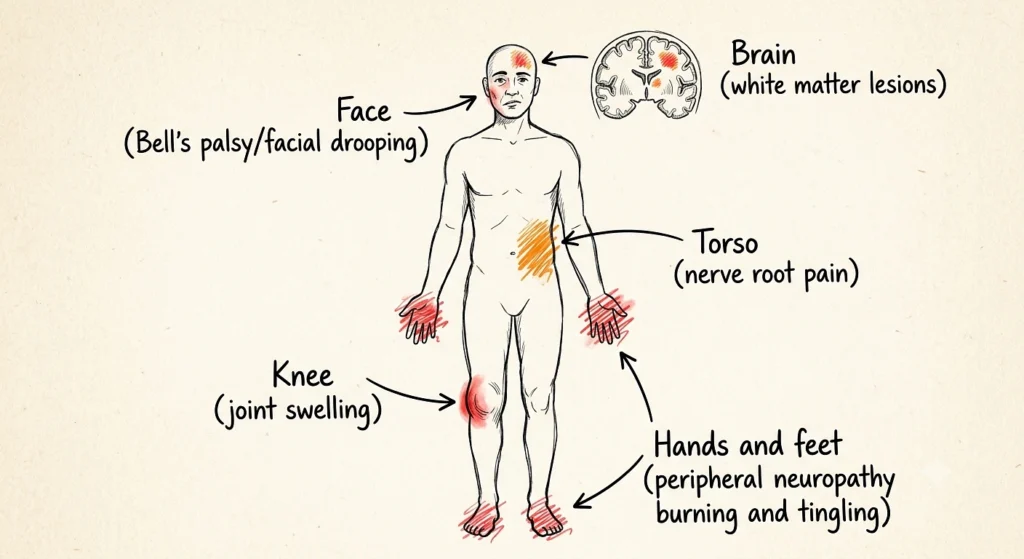
- Bell’s palsy or facial drooping. Lyme goes after cranial nerves, particularly the facial nerve. If you’ve ever had sudden weakness or drooping on one side of your face, Lyme should be in the conversation. Bilateral facial palsy – both sides affected, even at different times – is especially telling. It happens in Lyme. It’s rare in MS. If it’s in your medical record, somebody needs to connect it to those brain lesions.
- A knee that swelled up for no obvious reason. Lyme arthritis has a well-known preference for the knees, and it frequently shows up weeks or months before the bacteria pushes deeper into the nervous system. Maybe you saw an orthopedist about it. Maybe you iced it and moved on. Either way, if joint swelling came before brain fog and numbness, those events might belong to the same story.
- Burning or shooting pain in your hands and feet. Peripheral neuropathy – pain, tingling, burning in the extremities – is actually one of the most useful clues for sorting this out. And here’s why. MS only affects the central nervous system. Brain and spinal cord. Full stop. It does not damage peripheral nerves. So if you have peripheral neuropathy symptoms sitting right alongside white matter brain lesions, MS alone cannot explain both. Something else has to be going on. Lyme neuroborreliosis affects both central and peripheral nerves, so it can explain the full picture.
- Sharp nerve root pain radiating through the trunk or limbs. Radiculopathy – pain that follows a specific nerve distribution – is a recognized feature of neuroborreliosis, especially in European forms, and not a typical way MS presents itself.
- Time spent outdoors in tick-endemic areas. The high-risk zones in the US are the Northeast (Connecticut through Maine), the upper Midwest (Minnesota, Wisconsin), and parts of the Pacific coast. But Lyme has been reported in all 50 states and is endemic across Central Europe, Scandinavia, and the UK. If you’ve hiked, camped, gardened, or spent time in wooded and grassy areas, the exposure is plausible.
And before you say “but I’ve never had a tick bite” – about 50% of confirmed Lyme patients say the same thing. Nymph-stage ticks are the size of a poppy seed. Their bite is painless. They can attach, feed, and drop off without you ever knowing. Not remembering a tick bite tells your doctor exactly nothing.
Why the Standard Lyme Test Falls Short
This is the part that frustrates me every time I talk about it, because the testing situation is genuinely inadequate for neurological Lyme and a lot of doctors don’t realize it.
The CDC recommends two-tier testing. First, an ELISA blood screen for Lyme antibodies. If that comes back positive or borderline, a Western blot runs as confirmation. For early Lyme – someone with a recent tick bite and a bull’s-eye rash – this system works reasonably well.
For late-stage neurological Lyme, the wheels come off.
The ELISA misses patients with established infections because antibody levels fluctuate, and some people with longstanding disease don’t produce enough circulating antibody to cross the test’s positive cutoff. If that first-tier ELISA is negative, the Western blot never gets ordered – so the backup test never even enters the picture. And a small but documented group of patients with CSF-confirmed neuroborreliosis have completely negative blood tests. The infection is active in their nervous system and the serum testing doesn’t catch it.
One negative ELISA, drawn one time, does not reliably exclude neurological Lyme disease. That is not a fringe position. It’s a recognized limitation in the published infectious disease literature.
Tests That Actually Add Useful Information
When neurological Lyme is a real diagnostic consideration – not a wild guess, but a genuine possibility based on symptoms, exposure, and imaging pattern – these additional tests fill in what the standard blood work misses:
- CSF Lyme antibody index. Compares the ratio of Borrelia-specific antibodies in your spinal fluid versus your blood. A high CSF-to-serum ratio tells you the nervous system itself is producing antibodies against the bacteria. Strong evidence.
- C6 peptide ELISA. Uses a synthetic peptide from the Borrelia VlsE protein instead of the whole-cell preparation in the standard ELISA. Multiple studies show improved sensitivity for later-stage disease.
- CXCL13 levels in cerebrospinal fluid. This chemokine rises sharply during active neuroborreliosis and comes back down with successful antibiotic treatment. Useful for both initial diagnosis and tracking treatment response.
- PCR testing on CSF. Directly detects Borrelia DNA. Sensitivity is lower than antibody-based methods, but a positive result is highly specific – if the DNA is there, the bacteria is there.
Print This Checklist and Bring It to Your Doctor

If you’ve received a new MS diagnosis and any of the following apply to you, bring them up with your neurologist before starting disease-modifying therapy. Print this section out or screenshot it. Seriously.
- You’ve lived in or traveled to a Lyme-endemic region with outdoor exposure – Northeast US, upper Midwest, Pacific coast, Central Europe, Scandinavia, UK.
- You had unexplained joint swelling – especially a knee – at some point before the neurological symptoms started.
- You’ve had Bell’s palsy or facial weakness, particularly bilateral involvement.
- You have peripheral neuropathy symptoms – burning, tingling, shooting pain in hands or feet – alongside your brain lesions.
- Your MRI lesions are mostly subcortical without the classic periventricular distribution or Dawson’s fingers.
- Your spinal tap came back without oligoclonal bands.
- Lyme was never tested at all, or the only test was a single ELISA that came back negative and nobody followed up.
- You don’t recall a tick bite. Neither do half of all confirmed Lyme patients. It means nothing.
Ask your neurologist one direct question: “Has Lyme disease been properly excluded?” If the answer comes down to a single blood test, that’s not proper exclusion. Ask for a lumbar puncture with Lyme-specific CSF evaluation.