


{kind=link}
Most people meet Dupuytren’s contracture as a lump. There’s a small, firm knot in the palm, usually near the base of the ring or little finger, and it sits there for months or years doing very little. It doesn’t hurt, it doesn’t catch on anything, and so the natural assumption is that the lump is the disease and that getting rid of it is the goal. That assumption causes a lot of needless worry and the occasional needless surgery. The lump is almost never the thing that matters. What matters is the day your hand stops lying flat on a table.
The Lump Isn’t The Disease, The Cord Is
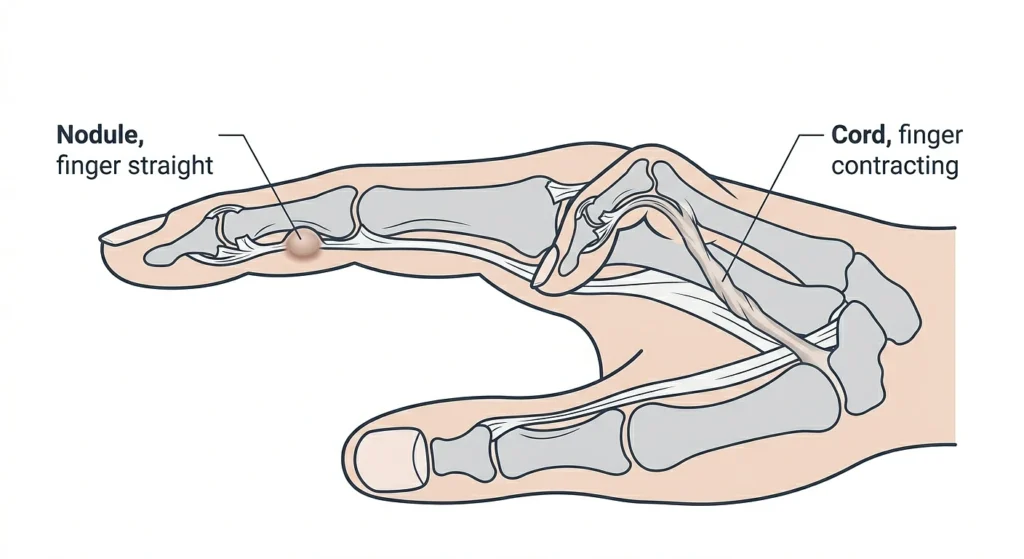
To see why, it helps to know what’s happening under the skin. Dupuytren’s is a slow thickening of the fascia, the sheet of connective tissue beneath the palm. Cells called myofibroblasts start laying down collagen along the natural lines of tension in the hand, and over time that deposit organizes into a cord. A nodule is inert. A cord is not. As it matures it shortens, and because it runs the length of the finger, that shortening pulls the finger down into the palm the way a tightening rope draws two points together. The ring and little fingers go first because the cords track along those rays. Stripped down, the whole disease is that: a rope forming under your skin and slowly reeling a finger in.
This is the one distinction worth holding onto. A nodule that bends nothing can be left alone indefinitely, and usually should be. A cord that has bridged a joint is a mechanical problem that won’t resolve on its own. So the real question isn’t whether you have Dupuytren’s, because plenty of people have it and never need a thing done. The question is whether a cord has begun locking a joint, and there’s a simple way to find out.
The Ten-Second Test You Can Run At Home
The test is older than most people reading this. An Australian surgeon, J. T. Hueston, described it in 1982, and it has survived four decades because nothing simpler has beaten it. You lay your hand palm-down on a table and try to press it completely flat, fingers straight. If the whole hand settles, you pass. If a finger stays bent and lifts the palm or fingertip off the surface, you fail, and that failure is a positive tabletop test.
Discomfort and a clear positive usually show up once the bend reaches around fifteen degrees, a figure the European orthopedic literature has pinned down. You can run this yourself tonight on any flat surface in the house, and it sorts you far more reliably than staring at the lump ever will: hand still flattens with a nodule present, watch it; hand won’t flatten, see a hand specialist.
A published case shows how literally this plays out. A man of sixty-three presented with an obvious cord and a finger he could no longer straighten, and what triggered his referral wasn’t the size of the cord or how long he’d had it. It was that he couldn’t lay his palm flat on the exam surface. The clinician measured his joint angles with a goniometer, confirmed the cord was the cause, and referred him on. The flat palm did the deciding.
Why The Joint Matters More Than The Bend
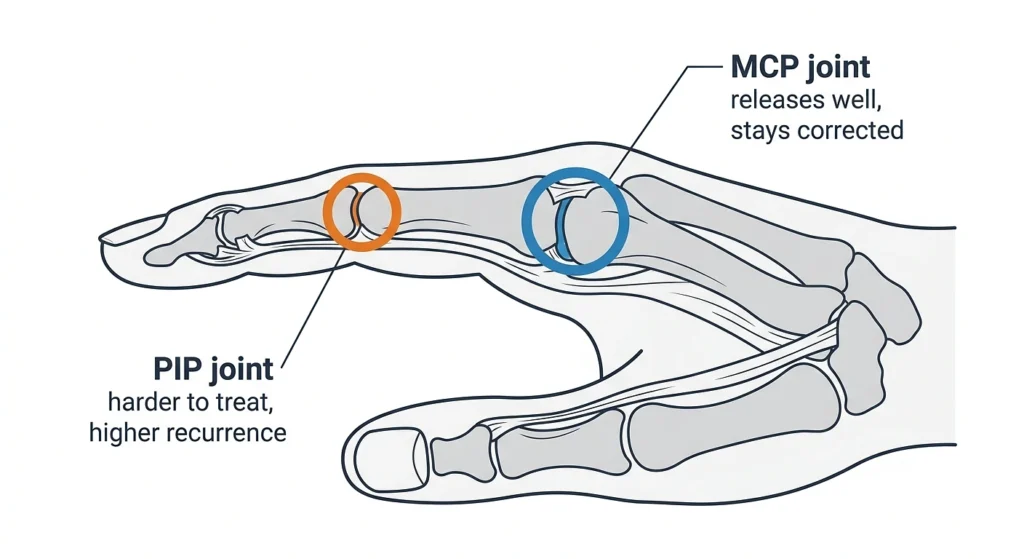
Once you’re past that point, the next question is narrower than most patients expect, and it shapes everything. It isn’t “how bad is it.” It’s which joint the cord is crossing. There are two candidates and they behave like different diseases.
The MCP Joint Is The Cooperative One:
The big knuckle where the finger meets the palm, the MCP joint, releases well under treatment and tends to stay released. It’s the one nobody loses sleep over.
The PIP Joint Is The One That Comes Back:
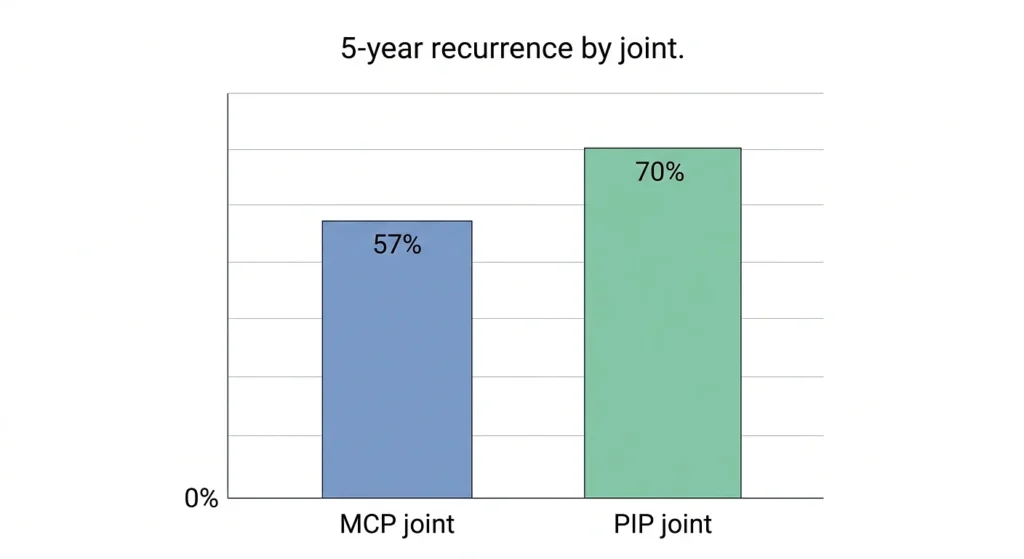
The middle joint of the finger, the PIP, is the one that gives surgeons grief, harder to straighten, sitting close to the digital nerves, and prone to returning. The recurrence numbers make the gap plain. One cohort following needle fasciotomy out to five years found the contracture came back in 57 percent of MCP joints and 70 percent of PIP joints. Same procedure, worse odds the moment the harder joint is involved.
That asymmetry is also why the referral thresholds look lopsided. The family-medicine guidance sends a patient onward at a thirty-degree contracture in the MCP, but at any degree at all in the PIP. That’s not arbitrary. The PIP punishes delay, so you move on it earlier even when the visible bend is smaller.
The Three Roads, And What Each One Costs You
This is the one place worth laying out side by side, because people genuinely compare these the way they’d compare cars:
- Needle aponeurotomy – The cord is weakened with a needle and snapped. Outpatient, quick recovery, best for MCP cords under about twenty degrees. The weakness is durability: recurrence runs 74 to 85 percent at five years.
- Collagenase injection – An enzyme dissolves the cord, straightening close to nine in ten MCP contractures to nearly flat within a week. Most people get some swelling and bruising afterward, common but short-lived.
- Limited fasciectomy – The cord is surgically removed. Lowest recurrence of the three and still the standard for advanced or recurrent disease, paid for with the longest recovery.
Which road fits depends heavily on the joint, the severity, and honestly how much recurrence a given person is willing to trade against downtime.
But My Hand Still Works. Do I Need To Do Anything?
A lot of the time, no. There is no cure for Dupuytren’s, only correction. Every procedure on that list fixes the bend without removing the underlying disease, which means every one carries a real chance of return. Putting a functional hand through a procedure can buy you a recovery period and a recurring contracture and little else.
What genuinely shifts the calculus is interference and momentum a finger that snags going into a pocket, a palm you can’t plant to push yourself out of a chair, a bend clearly worse than it was a few months back. The presence of the disease isn’t a reason to act. The disease taking something from you is.
References:
- Hueston, J. T. (1982). The Table Top Test. The Hand.
- Walthall, J., Anand, P., Rehman, U. H. (2023). Dupuytren Contracture. StatPearls, NCBI Bookshelf.
- Grazina, R., et al. (2019). Dupuytren’s disease: where do we stand? EFORT Open Reviews.
- Stallard, K. J., et al. (2019). Dupuytren’s contracture: Concise approach to an enigmatic condition. International Journal of Academic Medicine.
- Likelihood of Dupuytren Contracture Recurrence After Limited Fasciectomy, Needle Aponeurotomy or Collagenase Clostridium histolyticum (2026). Journal of Hand Surgery Global Online.
- Collagenase injection versus limited fasciectomy surgery (DISC). NIHR/NCBI Bookshelf.