


{kind=link}
Overview
- The lower back teeth and the ear share a nerve, so pain from an erupting molar is routinely felt, and misdiagnosed, as an ear infection.
- The danger window is 13 to 19 months, when the largest molars cut through at the same age ear infections naturally peak.
- A Finnish trial found restricting dummy use to sleep only cut ear infections by 29 per cent.
- Bedtime bottles drunk lying flat feed both tooth pain decay through the same drainage route.
- Before accepting another antibiotic: check the mouth, note whether a cold came first, and ask what the eardrum actually showed.
- Fever above 39°C, discharge, swelling behind the ear, or any sign the child cannot hear you.
One Nerve Serves Both The Molars And The Ear, And That Is Where The Confusion Starts
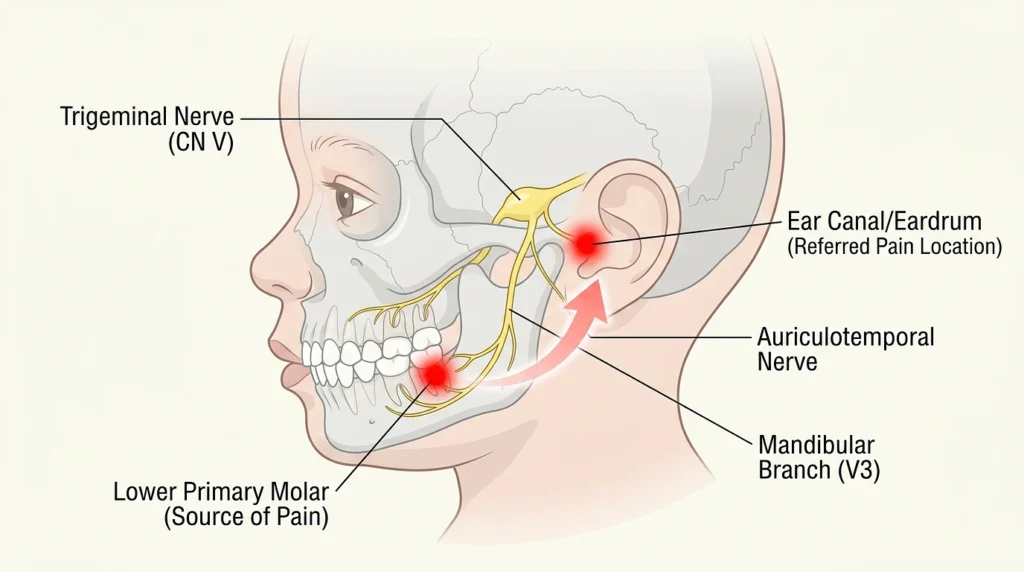
The lower teeth are innervated by the mandibular branch of the trigeminal nerve. One of its branches, the auriculotemporal, provides some of the innervation to the auditory canal and tympanic membrane. If a molar appears through the inflamed gum tissue, it can cause pain in the brain to be perceived as coming from the ear. This is known as referred otalgia, and is a known cause of ear pain in adults with a normal ear drum.
In a toddler, the picture is messier. They pull at the ear because that is where the pain feels like it lives. Add the mild fever, drooling, and night waking that come with molar eruption, and you have a near-perfect imitation of acute otitis media. A slightly pink eardrum, which is common in any crying, feverish child, is often enough to tip the diagnosis and trigger a prescription.
The cost of getting this wrong is not trivial. NICE guidance already pushes against routine antibiotics for ear infections because most cases clear within three days without them. A child treated three or four times for phantom infections has absorbed several unnecessary antibiotic courses, with the gut disruption and resistance risk that come with them, while the actual source of the pain was never examined.
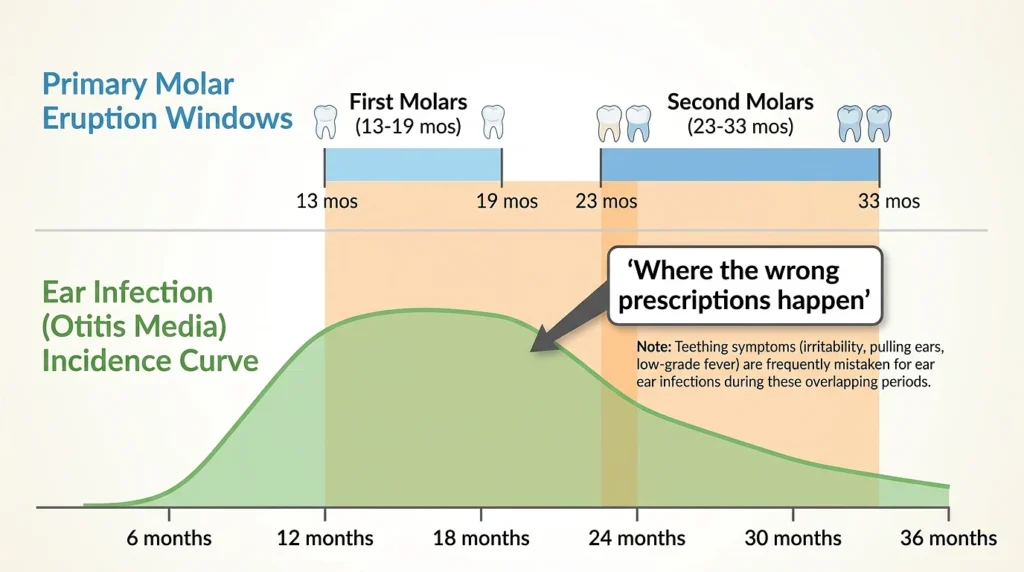
The 13 To 19 Month Window Is Where Most Of The Wrong Prescriptions Happen
Two timelines collide in the second year of life, and almost nobody plots them side by side.
First molars erupt between roughly 13 and 19 months, with second molars following between 23 and 33 months. These are the largest, slowest, most painful teeth a child cuts. At exactly the same age, ear infections hit their natural peak. Around 80 per cent of children have at least one ear infection by their third birthday, with the highest incidence between six and 24 months, partly because a toddler’s Eustachian tube is short, soft, and nearly horizontal, so it drains poorly.
So the months when the pain from the molars is most likely to be referred to the ear are the same months when it is most likely to have a genuine ear infection. If a clinician sees a feverish 16 month old with a ear tugging ear ache, he is, statistically speaking, almost guaranteed to make the correct diagnosis, which is otitis media. In the recurring cases the miss occurs. If the same child comes back each 5 or 6 weeks with the same symptoms and the eardrum doesn’t seem to be dramatically infected, then the eruption chart will be a better input into the prescription pad than the child’s symptoms.
A useful tell for parents: genuine acute otitis media usually follows a cold, because the infection travels up from the nose and throat. Ear pain that arrives without any preceding runny nose or cough, in a child who is drooling heavily and chewing on everything, points towards the mouth far more often than the ear.
The Dummy Link Is Real, And A Finnish Trial Put A Number On It
There is a second, entirely separate route from mouth to ear, and this one involves genuine infections rather than referred pain.
Researchers in Finland ran a trial across well-baby clinics in Oulu, where parents in the intervention group were counselled to restrict dummy use to the moments of falling asleep only. The result, published in Pediatrics in 2000, was that acute otitis media fell by 29 per cent in the restricted group compared with families who carried on as usual. Earlier work by the same team had already found that continuous dummy users under two had measurably more ear infections than non-users.
It’s mechanical. The continuous sucking causes pressure changes in the nasopharynx, which may help to clear fluids from the back of the throat to the Eustachian tube’s opening. When a dummy falls to the floor, gets a quick wipe and goes back in, the bacteria are also carried straight to the same junction.
The same habit damages the teeth on a parallel track. Prolonged dummy use past the age of two is associated with anterior open bite and changes to the palate shape. So the dummy is quietly working on both problems at once, and the family hears about the teeth from the dentist and the ears from the GP, with neither professional connecting the two.
The practical move is not banning the dummy overnight. The Finnish protocol was modest: dummy only for settling to sleep, removed once the child is asleep, gone entirely after the first year if possible. That alone produced the 29 per cent drop.
Bottle Propping Feeds Decay And Ear Infections Through The Same Channel
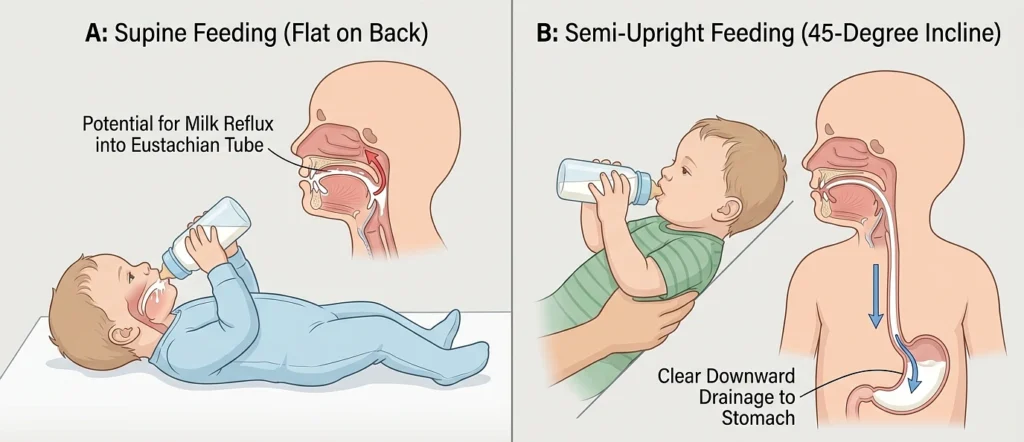
The third connection is the bedtime bottle, drunk lying flat.
There are two things that occur when a toddler drinks milk while lying down. The common pattern of caries around the upper front teeth, that used to be referred to by dentists as ‘bottle rot’, is what milk causes. At the same time, the swallowing position is flat so that any liquid and the bacteria it carries reflux up toward the Eustachian tube openings; in a toddler, the eustachian tube openings are located close to the mouth (not above it).
Feeding position shows up repeatedly in otitis media risk research for exactly this reason, and it is one of the few risk factors a parent can change tonight at zero cost:
- Feed at an incline of roughly 45 degrees, never flat on the back or in the cot.
- Finish the bottle before sleep, then water only if the child genuinely needs a drink overnight.
- Move to an open cup from 12 months, which UK dental guidance recommends anyway for the sake of the teeth.
A family that fixes the bedtime bottle often sees both problems ease at once, which is itself a strong hint that the two were never separate problems to begin with.
What To Check Before Accepting The Next Antibiotic Prescription
None of this means refusing treatment for a real infection. It means arriving at the appointment with better information than “she keeps getting ear infections.”
- Look in the mouth first. Swollen, bluish, or torn gum over the back of the jaw on the same side as the ear-pulling is significant. Mention it.
- Track the pattern against the eruption chart. If flare-ups cluster around the 13 to 19 month and 23 to 33 month windows and skip the months in between, say so.
- Note whether a cold came first. No preceding congestion makes referred dental pain more likely.
- Ask what the eardrum actually showed. A bulging, immobile, clearly infected drum justifies treatment. “A bit pink” in a crying child does not, and it is reasonable to ask which one the doctor saw.
- Audit the dummy and the bottle. If either habit is in daily use, you have two evidence-backed changes to make before assuming the child is simply unlucky.
When It Really Is The Ear
The caution cuts both ways, and this is where some parents overcorrect. Baby teething has been blamed for childhood fevers for two centuries, and the habit of attributing everything to teeth has its own casualty list. A genuine ear infection that goes untreated in a high-risk child can progress, and repeated true infections with lingering fluid, the condition known as glue ear, can dull hearing during the exact window when speech is developing.
Treat these as non-negotiable red flags regardless of any teething evidence: fever above 39°C, fluid or pus draining from the ear, symptoms lasting beyond three days, a child who seems not to hear you, or any swelling behind the ear. Those belong to the GP the same day.
The point is not that teeth cause every ear problem. The point is that in the second year of life, the mouth and the ear share a nerve, a drainage junction, and a set of household habits, and a recurring pattern deserves an explanation that accounts for all three rather than another seven-day course of amoxicillin and a hope for the best.