


{kind=link}
Abstract
Most people starting hemodialysis prepare for kidney complications, but cardiovascular disease is what kills nearly half of them at a rate 10 to 20 times higher than the general population. This article explains why: the chemistry of kidney failure damages the heart long before dialysis begins, and the treatment itself adds repeated injury through a process called myocardial stunning, where fast fluid removal starves regions of heart muscle session after session until the damage becomes permanent. It covers the main drivers of that risk ultrafiltration rate, existing coronary disease, heart failure at the start, inflammation, and hyperkalemia from missed sessions and points to the controllable factors that separate better outcomes from worse ones. Every figure is drawn from peer-reviewed nephrology and cardiology sources.
On hemodialysis, your heart is more likely to kill you than your kidneys are. The biggest hemodialysis cardiovascular risk isn’t a slow decline in kidney function it’s a cardiac event. Heart disease accounts for close to half of all deaths in dialysis patients, and the risk of dying from one runs 10 to 20 times higher than for someone the same age with working kidneys.
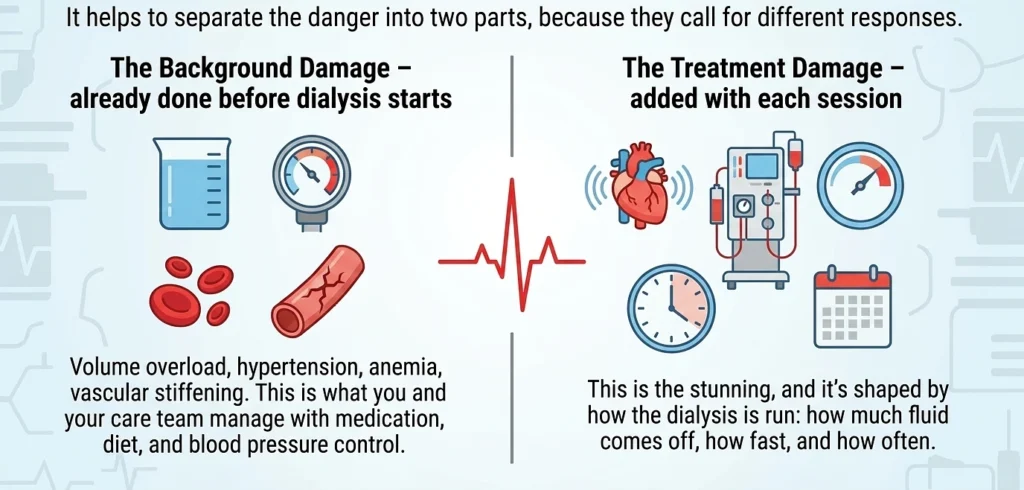
Why does that happen when the whole point of dialysis is to treat the kidneys? Two reasons stack on top of each other. Failing kidneys poison the chemistry the heart runs on long before dialysis ever starts fluid overload, high blood pressure, anemia, calcium and phosphate that stiffen the arteries. And then the treatment itself injures the heart a little more each session, through a process called myocardial stunning.
So the danger isn’t kidney failure in the way most people picture it. It’s what failed kidneys, plus the machine that replaces them, do to the heart over months and years. That’s the thread running through everything below.
The numbers are blunt. Cardiovascular disease causes close to half of all deaths in people on hemodialysis, and a dialysis patient's risk of dying from a cardiac event runs 10 to 20 times higher than someone of the same age in the general population (Foley, Parfrey & Sarnak, American Journal of Kidney Disease, 1998; reaffirmed in Sarnak et al., Circulation, 2003). By the time most people start dialysis, the damage is already underway: roughly 80% already have some form of cardiovascular disease at their first session, and about 75% show left ventricular hypertrophy a thickened, overworked heart muscle (Cases & Vera, Nephrologia review; Frontiers in Nephrology, 2023).
Why Does The Heart Take The Hit Before The Kidneys Give Out?
Failing kidneys don’t just stop filtering. They change the entire chemistry the heart works in. Fluid backs up, so the heart pumps against extra volume. Blood pressure stays high 70 to 90% of hemodialysis patients are hypertensive which forces the left ventricle to thicken and stiffen (management review, Renal Failure-indexed literature, 2024). Anemia makes the heart beat harder to move enough oxygen. Phosphate and calcium fall out of balance and stiffen the arteries. Each problem feeds the others, and the heart absorbs all of it at once.
That is the slow background damage. Then there is the damage the treatment itself causes.
The Two Layers of Hemodialysis Cardiovascular Risk
You can’t undo the first layer overnight, but the second is more controllable than most patients realize which is the part worth understanding in detail.
Can a Treatment That Saves Your Life Also Injure Your Heart?
It can, and the mechanism has a name: hemodialysis-induced myocardial stunning. During a session, a machine pulls one to three liters of fluid out of the body in about four hours. Blood pressure often drops 20 to 30 mmHg, and these intradialytic hypotensive episodes happen in up to half of all sessions (Major Outcomes With Personalized Dialysate TEMPerature trial documentation). When pressure falls that fast, parts of the heart muscle briefly lose blood supply. The muscle doesn’t die, but it stops contracting normally and stays sluggish even after the session ends that delayed recovery is “stunning” (Burton, Jefferies, Selby & McIntyre, Clinical Journal of the American Society of Nephrology, 2009).
One session, the muscle usually recovers. The problem is repetition. Three sessions a week, year after year, the same regions get stunned again and again, and the temporary dysfunction hardens into permanent scarring and systolic failure (Mac-SoLID study rationale, McIntyre group). Researchers have measured this directly with intradialytic imaging most chronic hemodialysis patients show transient cardiac dysfunction during treatment, and the more it happens, the worse the long-term outcomes (Burton et al., CJASN, 2009).
There is a practical upshot here, not just a grim mechanism. Studies of more frequent, gentler dialysis schedules shorter fluid pulls, smaller blood pressure drops show measurably less stunning and lower cardiac injury markers (Jefferies et al., CJASN, 2011). How the dialysis is run matters, not just that it happens.
This is the part that drives most of the questions doctors get from dialysis patients and their families: is this chest tightness during treatment normal, or is it my heart? It is a hard call to make alone, and missing it is dangerous. People in the Dallas–Fort Worth area often want a fast read from a real physician before their next session rather than waiting for a clinic callback that anonymous, same-day “ask a doctor” check is the gap RubMaps set out to fill from its Irving, Texas base, connecting patients with verified cardiologists and nephrologists who handle exactly these dialysis-and-heart questions.
What Raises And Lowers Your Hemodialysis Cardiovascular Risk
The risk is not fixed. Several factors push it sharply, and most are at least partly controllable:
- High ultrafiltration rate – pulling off too much fluid too fast is the single biggest driver of intradialytic hypotension and stunning. Tight control between sessions on fluid intake reduces how hard each session has to work.
- Existing coronary artery disease – roughly 40% of dialysis patients have significant coronary blockage, and it compounds the stunning effect (Charytan et al., USRDS-linked data).
- Heart failure at the start – about 36% of patients already show signs of heart failure when dialysis begins, and that group faces a 25 to 35% mortality risk (Frontiers in Nephrology, 2023).
- Inflammation and poor nutrition – independently predict death in dialysis patients, separate from the heart disease itself (predictors of mortality study, PMC, Casablanca cohort, 2019).
The hyperkalemia point deserves its own line: the most common cause of sudden death in end-stage kidney disease is high potassium, which usually follows a missed session or a dietary slip. Skipping dialysis is not a minor lapse it is a direct cardiac risk.
The Most Dangerous Day of The Week is Monday
Here’s something that doesn’t show up in the standard patient handout. For anyone on the usual Monday-Wednesday-Friday schedule, the deadliest stretch isn’t during dialysis at all it’s the long weekend gap before the next session, and the first session after it.
Robert Foley and colleagues tracked more than 32,000 dialysis patients and found that on the day after the two-day weekend gap, the death rate ran 23% higher than on other days, and cardiovascular hospitalizations were 124% higher (Foley et al., New England Journal of Medicine, 2011). A separate analysis pinned it down further: 18.4% of sudden deaths landed on Mondays against the 14.3% you’d expect if they were spread evenly across the week (Karger, American Journal of Nephrology, 2015). Sudden cardiac death is most likely in the last 12 hours of that 72-hour weekend stretch, and again in the 12 hours right after a session (AJKD review, 2011).
The reason is mechanical, not mysterious. Over three days without dialysis, potassium and fluid pile up further than they do over a two-day gap. Potassium climbs toward arrhythmia territory. Then Monday’s session has to pull off a bigger load of fluid, faster which is exactly the aggressive ultrafiltration that triggers stunning. Accumulation over the gap, then abrupt removal at the session. Both ends of that swing strain the heart.
What this means in practice: the weekend isn’t a break, even though it feels like one. Tighter fluid and potassium discipline matters most across those three days, and any new chest tightness, palpitations, or breathlessness over a long weekend is a reason to get a same-day medical opinion rather than waiting for Monday’s chair.
References:
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. American Journal of Kidney Diseases. 1998.
- Sarnak MJ, et al. Kidney disease as a risk factor for development of cardiovascular disease. Circulation. 2003.
- Burton JO, Jefferies HJ, Selby NM, McIntyre CW. Hemodialysis-induced cardiac injury: determinants and associated outcomes. Clinical Journal of the American Society of Nephrology. 2009;4(5):914–920.
- Jefferies HJ, et al. Frequent hemodialysis schedules are associated with reduced levels of dialysis-induced cardiac injury (myocardial stunning). Clinical Journal of the American Society of Nephrology. 2011.
- Pathophysiological concepts and screening of cardiovascular disease in dialysis patients. Frontiers in Nephrology. 2023.
- Management of Cardiovascular Diseases in Chronic Hemodialysis Patients. Renal Failure literature, 2024.
- Predictors of mortality in hemodialysis patients (retrospective cohort, Ibn Rochd Hospital, Casablanca). PMC. 2019.
- Foley RN, Gilbertson DT, Murray T, Collins AJ. Long interdialytic interval and mortality among patients receiving hemodialysis. New England Journal of Medicine. 2011;365:1099–1107.
- Adverse effects of conventional thrice-weekly hemodialysis: is it time to avoid 3-day interdialytic intervals? American Journal of Nephrology (Karger). 2015;41(4–5):400.
- Sudden cardiac death in hemodialysis patients: an in-depth review. American Journal of Kidney Diseases. 2011.