


{kind=link}
A man’s in the clinic chair, leg braced ankle to thigh, cigarette between his fingers, and there’s already a small pile of butts in the ashtray beside him. The X-ray shows why he’s here a clean break across the tibial shaft, the two ends just slightly out of line. He told the surgeon he’d quit. The ashtray disagrees.
Surgeons see this constantly. What a patient says about smoking is some of the least reliable information in the whole workup, and when the break is in the tibia, that unreliability costs more than it would almost anywhere else.
Quick Reference:
| Nicotine | Cotinine | |
|---|---|---|
| Half-life | ~30–60 min | ~11–37 hr |
| Detection window | A few hours | ~2–3 days (urine); full clearance up to ~10 days |
| Sample types | Blood, saliva | Urine, serum, saliva |
| Active smoker (saliva) | — | >100 ng/mL |
| Passive exposure (saliva) | — | <5 ng/mL |
| Best for | Very recent use only | Confirming recent exposure |
Why “I Quit” Doesn’t Settle It
The tibia heals badly. That long border sitting just under the skin gives it a poor blood supply to start with, so it already drifts toward slow union and nonunion before you add a single complicating factor. Nicotine is the factor that pushes it over.
It comes down to circulation. Nicotine drives a catecholamine release, the vessels constrict, perfusion drops. The bone loses the oxygen and the inflammatory cells it needs most in those first weeks angiogenesis falters, the early healing cascade stalls, the bone-building cells don’t arrive in the numbers required. Separately, Detection of nicotine metabolites interferes with osteoblast function and blunts the immune response, which is a large part of why smokers get more infections.
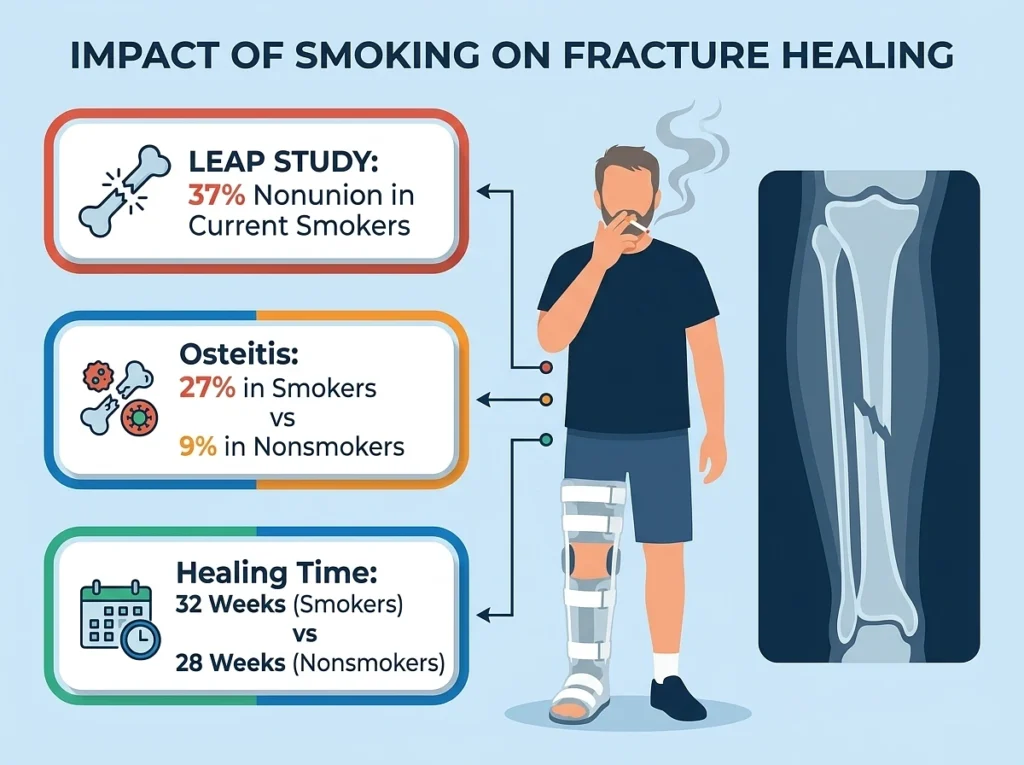
The numbers aren't subtle. The LEAP study put nonunion at 37% in current smokers and 32% in former smokers, with osteomyelitis well above baseline in both groups. One open-tibial-fracture cohort recorded osteitis in 27% of smokers against 9% of nonsmokers. Another found smokers with open and high-grade bone fractures took roughly 32 weeks to heal versus 28 for nonsmokers.
A truthful quit and a convenient one describe two different recoveries. That’s the whole reason a surgeon won’t just take the claim the answer shapes the timeline, the hardware, and how hard the union gets watched.
Why You Don’t Test For Nicotine
Its half-life is about an hour after a cigarette, so a man who smoked yesterday morning reads clean by the time you draw blood. The negative tells you almost nothing genuine abstinence and a cigarette three hours ago look identical. For a question that spans days and weeks, a marker gone in under two hours is useless.
Cotinine:
Cotinine is what nicotine becomes, and the body holds it far longer a half-life of 11 to 37 hours against roughly 30 minutes. The liver converts 70 to 80% of nicotine into it, so there’s plenty around and it lingers.
That’s the entire advantage. In urine at a 200 ng/mL cutoff, cotinine stays detectable for two to three days, and it reads from urine, serum, or saliva. Labs use it to check self-reported smoking for exactly this reason: it catches what the interview misses. It barely moves across the day, so the timing of the draw doesn’t change the result.
Nicotine tells you whether someone smoked in the last hour or two. Cotinine tells you whether they’ve had in the last few days. Only the second question is worth asking when the patient is insisting he’s done.
Reading the number:
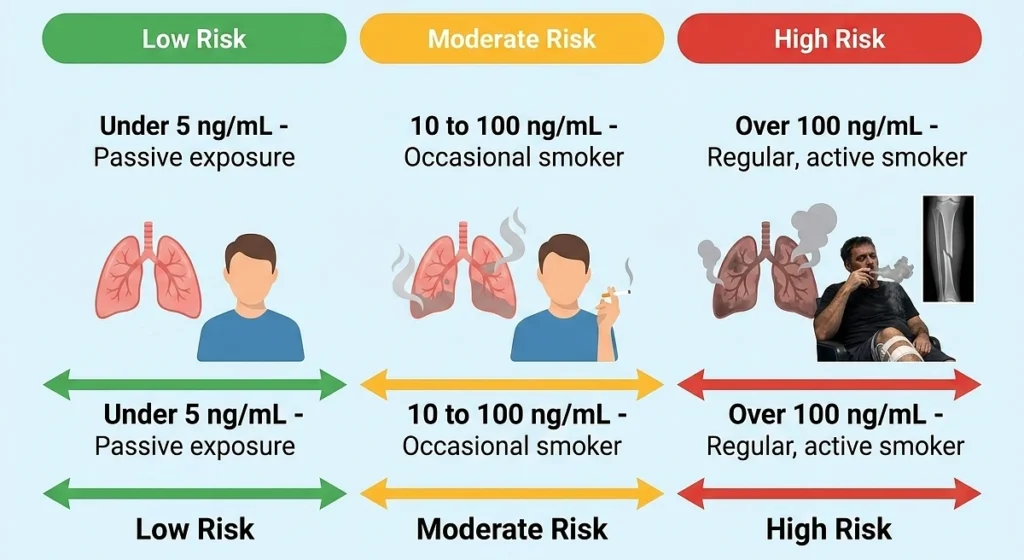
A cotinine result isn’t binary. The level itself separates an active smoker from trace second-hand exposure. In saliva it sorts out roughly:
- Under 5 ng/mL — passive exposure, someone around smoke rather than smoking it.
- 10 to 100 ng/mL — an occasional smoker, or a regular one on low-nicotine cigarettes.
- Over 100 ng/mL — a regular, active smoker.
Someone who actually quit two weeks ago reads low or clear. Someone still working through a pack a day lands up high regardless of what he said at the desk. That’s where the test earns its keep.
How Long Ago Does He Have To Have Quit?
The natural follow-up, and the place two things get confused detection window versus full clearance. The two-to-three-day urine figure is just how long cotinine reliably trips a standard cutoff. Clearing it entirely takes longer, up to about ten days in regular users, and that number moves with genetics, how much someone smoked, and the product they used. Menthol smokers hold onto it longer still, as do people regularly around menthol smoke.
So a borderline result wants interpretation. A low-but-present level might be someone several days out from quitting and still washing it through not someone smoking daily. The concentration carries the story, not the bare positive.
When Doing The Right Thing Still Fails The Test
Cotinine can’t tell the source apart. Cigarettes, vaping, dip, gum, the patch all the same reading. So the patient wearing a nicotine patch to get off cigarette smoking, doing precisely what you asked, tests positive.
It’s not a false positive. The nicotine is genuinely there, and it isn’t clinically irrelevant, because what transdermal does to a healing fracture isn’t established not shown safe, just not studied enough to rule out the same vasoconstriction problem. A positive in that patient isn’t a gotcha, it’s a reason to find out what form of nicotine you’re dealing with and whether it’s still working against the bone. And since the CYP2A6 enzyme varies between people and changes how fast clears, you’re making a judgment call rather than reading against a fixed line.
What It Changes
Confirming exposure only matters if it moves the plan. In a tibial fracture, a positive cotinine usually feeds a few decisions:
- A real cessation conversation, ideally a referral quitting is the largest lever the patient still holds, and former smokers heal better than current ones, which says some of that vascular function returns.
- A reset timeline, expecting slower union and watching for early delayed-union signs instead of assuming a clean course.
- Tighter follow-up imaging, because nonunion in a smoker’s tibia is common enough that catching it early keeps the options open.
- Hardware and counseling choices weighted toward the higher infection and nonunion risk the number just confirmed.
The test heals nothing. It swaps the patient’s word for a measurement, so the plan rests on what’s circulating rather than what got said in the waiting room.
References
- Influence of Smoking Status on Fracture Healing Time: A Retrospective Cohort Analysis — PMC (PMC12812234)
- Tobacco and Bone Fractures — Bone & Joint Research, 2019
- Fracture Healing: How Strong Is the Effect of Smoking on Bone Healing? — Clinical Gate / LEAP Study data
- One Step Cotinine Test, Package Insert — Thermo Fisher
- Assessment of Smoking Status Based on Cotinine Levels — Tobacco Induced Diseases (PMC2711055)
- Biomarkers of Cigarette Smoking — Benowitz, NCI
- Detection of Nicotine Metabolites (saliva concentration tiers) — biosensor patent literature
- How Long Does Nicotine Stay in Your System — Drugs.com, 2025
- The Cotinine Test for Tobacco Use — Podiatry.com, 2025