


{kind=link}
A red dot on your chest, pinhead-sized, and you’re fairly sure it wasn’t there last year. Sometimes there’s just one. Sometimes a few, scattered down your torso or sitting somewhere on your back you can’t really see. They don’t itch. They don’t hurt. They’re just there.
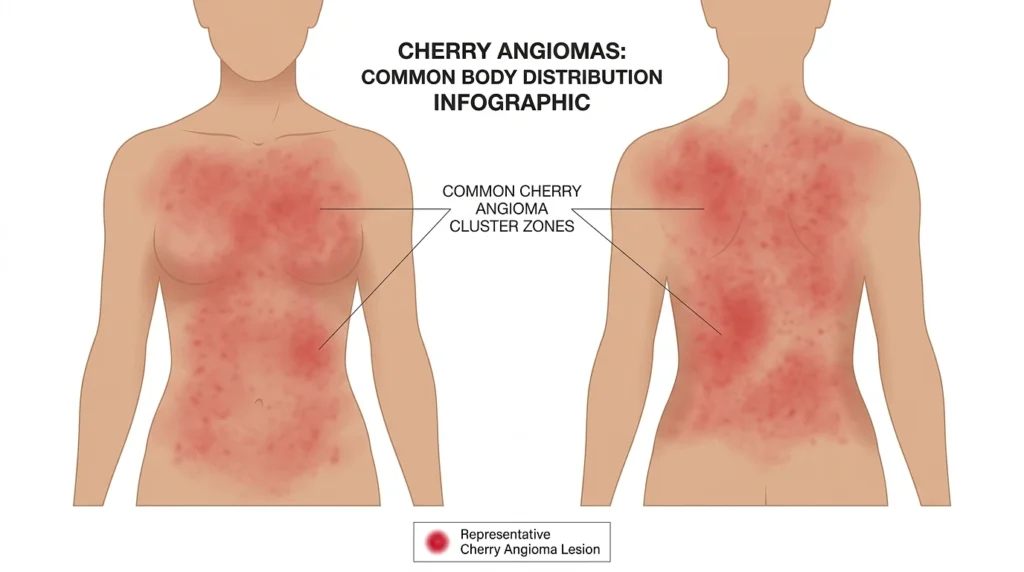
Usually these are cherry angiomas. They’re the most common harmless blood-vessel growth adults get, and the trunk is where they like to sit, the chest mostly, then the back.
The thing driving them is age, not illness. People start getting them after about 30, and the number goes up from there. By 75, around three in four adults have at least a couple. Men tend to have more than women. A full-body imaging study counted a median of 16 in men and 12 in women, and the spots got bigger as well as more numerous as people aged. They don’t turn into cancer. The cause sits down at the cellular level, in mutations to two genes, GNAQ and GNA11, that show up inside a lot of these growths.
What a Cherry Angioma Actually Is
It’s a small knot of blood vessels bunched up near the surface of the skin. That’s the whole thing. The blood in it is what you’re looking at, and the color shows through, which is why most of them read red. Some look purple, a few almost blue. Depends how deep they sit and how the light hits.
They start flat and tiny. Over months or years some stay flat and some rise into a little smooth dome. They run from pinhead-sized to about a quarter inch. The edge is what gives it away. Clean, round, defined, not the blurry spreading border you get from a rash.
Old textbooks call them Campbell de Morgan spots, after the Victorian surgeon who first wrote about them. The other name just won out.
Telling It Apart From the Lookalikes
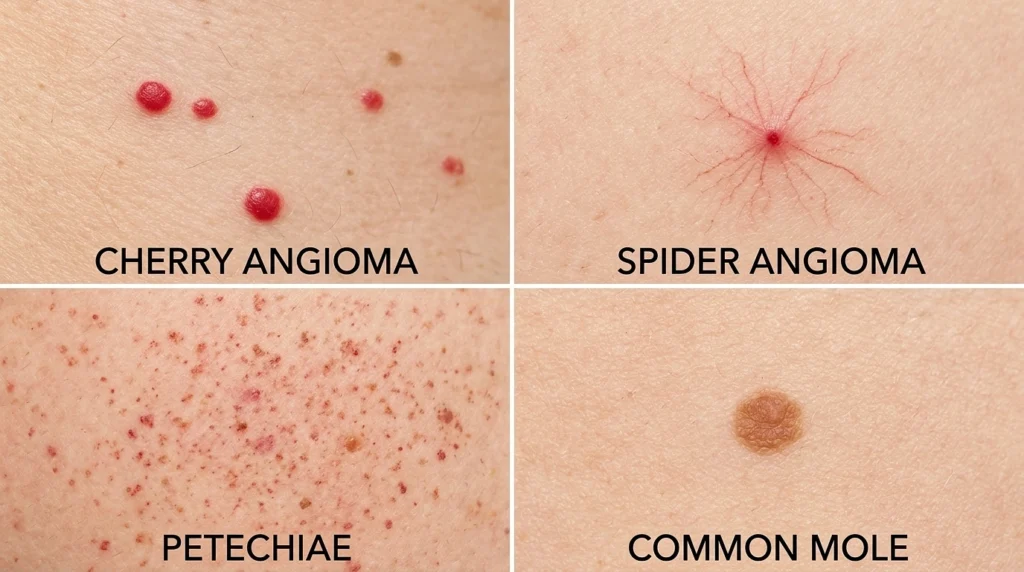
A red dot isn’t automatically a cherry angioma. A few other things look similar, and a couple of them are worth ruling out before you wave it off.
| Spot | Color | Texture | Blanches when pressed? | The tell |
|---|---|---|---|---|
| Cherry angioma | Cherry red to purple | Smooth, flat or domed | Usually no | Sits unchanged for years, clean round edge |
| Spider angioma | Red center, lines fanning out | Flat | Yes, fills back from the middle | The spider-leg branches |
| Petechiae | Tiny red-brown specks | Flat | No | Come on suddenly in clusters, get these checked |
| Mole | Brown, tan, pink | Flat or raised | No | Pigment, not blood, watch for asymmetry |
| Melanoma | Mixed, often dark | Irregular, may be raised | No | Changing, uneven, growing, see a doctor now |
There’s a home check that helps press on it. A cherry angioma usually stays red under your finger, because the vessels are a fixed little cluster, not blood that drains and refills. A spider angioma goes white and then fills back in from the center. That’s not a diagnosis. It just tells you whether you’re dealing with something to watch or something to ignore.
Why the Chest and Back
Nothing flips them on like a switch. A few things make them more likely, though.
- Age is most of it. They get more common after 30 and keep adding up decade by decade, so a seventy-year-old with a handful of them is completely normal. The chest, trunk, and back are just big patches of skin that have been around a long time, and that’s where these collect. In the imaging study, the front of the trunk came up most often, the back second.
- Sex matters a bit too. Same study, men had more than women, 16 against 12, and the spots grew in size and number with age.
- Genetics pull two ways. They run in families, so if a parent is covered in them, you’re more likely to get them. And underneath that, sequencing has found those GNAQ and GNA11 mutations in a lot of the growths, which is about as close to a mechanism as the research gets right now.
- Hormones come up a lot, usually pregnancy, because some people get a fresh batch while expecting and the hormone shift gets blamed. The evidence is weaker than people think. One study found no link at all between cherry angiomas and pregnancy, diabetes, or cholesterol problems. For most people it comes back to age, sex, and family.
Are They Dangerous?
Almost never. They’re benign. Not cancer, not turning into cancer. Somebody floated a cancer link back in the 1800s when these first got described, but it never panned out, and for a long time they were treated as nothing more than a sign of getting older. Having ten of them, by itself, means nothing.
There’s one melanoma footnote worth being straight about. A few studies found that people with ten or more had a higher melanoma rate, and the effect was strongest in people under 40. But those studies were retrospective and run inside melanoma clinics, so the patient pool was skewed from the start. The angiomas might just be along for the ride. Read it as a reason to stay on top of skin checks, not a reason to start counting dots.
What they do do, if you give them the chance, is bleed. They’re full of vessels and some of them stick up, so a razor or a fingernail or a zipper can catch one. It bleeds more than you’d expect for the size, and pressure sorts it out. The ones on your back are the easy ones to nick without realizing, because you can’t see them coming, and that’s often what makes people decide to get them off.
If One Starts Bleeding
- Hold firm pressure. A clean tissue or gauze on it, firm, for a full 5 to 10 minutes.
- Don’t lift it to look. Checking just starts it bleeding again.
- Once it’s done, leave it dry, or stick a small plaster on if that’s easier.
- If it won’t quit, 15 minutes of real pressure and it’s still going, or it keeps reopening, get it removed properly.
When a Red Dot Deserves a Second Look
Most are harmless. But skin is one place where it’s genuinely worth knowing which changes are the ones that matter. Get a spot looked at if:
- It changes color, shape, or size over a short stretch.
- It bleeds for no reason, with nothing touching it.
- The edge goes ragged or blurry instead of staying clean and round.
- It shows more than one color.
- It itches, crusts over, or won’t heal.
None of that fits a cherry angioma, and all of it lines up with warning signs for other things. A real one holds still, one even color, an edge you could draw with a compass. Anything that strays from that is worth a trained eye instead of a guess. And if you honestly can’t tell, that alone is reason enough to book an appointment. A dermatologist would much rather look at something harmless than miss the one that wasn’t.
Can You Get Rid of Them?

You don’t have to. Plenty of people keep theirs for life and never think about it again. But if one keeps bleeding, or sits somewhere it’s always getting caught, or you just don’t like looking at it, taking it off is simple.
- Laser collapses the vessels with a beam, and the spot fades over a week or two. Quick, and good for the flat ones.
- Electrocautery burns it off with a small current. Fast, usually after a numbing pinch.
- Shave removal slices it flat with a small blade, which suits the raised ones.
- Cryotherapy freezes it with liquid nitrogen, but it’s used less for these, because cherry angiomas sit a bit deeper than the surface spots freezing works best on.
The visit is dull, which is the point. The dermatologist looks at the spot first to make sure it’s actually a cherry angioma and not something that needs a biopsy. They clean it, and for a cautery or shave they numb it with a bit of local. The removal takes seconds to a couple of minutes a spot. You go home the same day, and most people get several done in one sitting.
After, keep it clean and dry for a day or two. A little scab or a pink mark is normal and fades over a few weeks. Don’t pick at it. The picking is what scars, not the procedure. Put sunscreen on the healed patch, because new skin health burns easier.
The one thing not to do is the home version, cutting or burning or freezing one off yourself. With that many vessels in such a small spot it bleeds more than you’d think, and you trade a clean result for a scar or an infection, for no reason. Two minutes with the right tools in a clinic. A bad idea over the bathroom sink.
This is general information, not a diagnosis. If a spot on your skin worries you, get a doctor or dermatologist to look at it in person.