

You’re on the same counter, the same hours, working on the same hard floor with a coworker. Your lower back by 3 PM: Aching, they’re not aching. The typical response is that they’re made tougher, younger or they haven’t worn them out yet.
According to the research, that is not the case. The only difference between those who develop back pain when standing and those who do not is that the former have a habit of not standing at all — not quite the opposite of what you’d think. Those who remain comfortable are constantly shifting their weight — little half-conscious fidgets, foot to foot all shift long. Your dependable fellow worker is not tougher. They’re on the move and you are in frozen mode.
The reason is mechanical, not mysterious. When you hold a posture, the same muscles and joints carry the same load with no relief, and the tissue starts complaining. Movement spreads the load around — every shift hands the work to a fresh set of muscles before the last set has had enough. Your coworker’s constant fidgeting is, without them knowing it, a built-in load-sharing system. Stand still and you switch it off.
That one idea runs underneath everything else here — the back pain, the shoe question, even the swollen legs and varicose veins that come with the territory. So it’s worth following all the way down.
The clock starts faster than anyone thinks
Most people picture standing pain as something that accumulates slowly across a long shift — fine at noon, sore by five. The lab data says otherwise. In controlled standing studies, clinically meaningful low-back pain shows up at around 71 minutes of prolonged standing, and in the people prone to it, that drops to about 42 minutes. One study on office workers put the threshold even earlier, finding that 30 minutes is roughly where back and foot pain begins to set in during a one-hour standing task.
Half an hour. Not a shift. That’s the one that you want to sit with, because you actually don’t wear out over 8 hours, you hit a wall in the first hour and then hit it again and again.
And this is the truly useful discovery below! Standers are divided into two groups: “pain developers” and “non-pain developers. Nearly half (44%) converted to pain developers in one 2-hour standing study. It wasn’t an age question or a weight question or a fitness question. It was movement.
What the comfortable people are actually doing
Lack of movement is the predisposing factor. Researchers tracking both the lumbar spine and the foot-ground interface found that the people who developed pain moved less — fewer weight transfers, fewer shifts in where their center of pressure sat over their feet. Early stillness, specifically, is the warning sign. The work even has a name for it: early static standing is associated with prolonged-standing-induced low back pain.
The people who stay fine keep loading and unloading the joint. They drift onto one hip, then the other. They rock slightly. They never let the same tissue carry the same load for long. That low-grade, constant redistribution is doing real protective work — and it’s mostly involuntary, which is why the comfortable coworker can’t tell you their secret. They don’t know they’re doing it.
The flip side is the uncomfortable truth about the most “sensible” fix. A 15-minute sit-down break sounds like the obvious cure. It isn’t, or at least not reliably. In one study using a 45-minutes-standing, 15-minutes-sitting ratio, the seated break failed to deliver lasting relief — pain climbed back, and after the break it returned to an even higher level once standing resumed. The pain developers tended to lock into rigid postures and move through a narrower range. The break didn’t fix the stillness. It just paused it.
So the mechanism, in one line: standing doesn’t hurt you. Standing still hurts you. And about half of all people are wired to go still under load without noticing.
It’s not just your back — your veins run on the same system
Here’s where the stillness problem stops being only about pain and starts being about something that can actually progress into a medical condition.
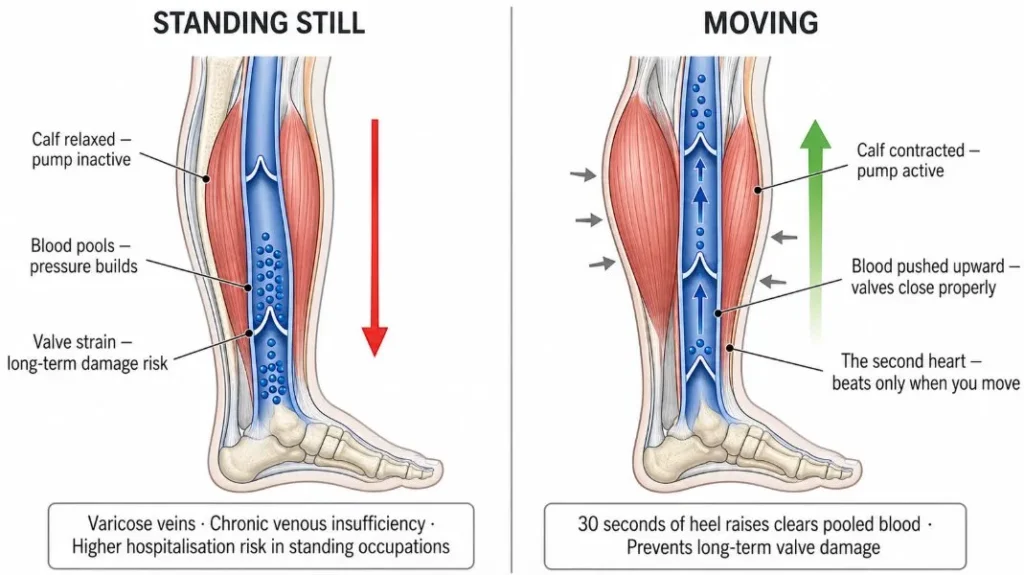
Blood flow in both veins of your legs is against the force of gravity back to the heart. Do not have their own pump. They borrow one, the calf muscles. Each contraction of the calf compresses the deep veins and pushes the blood up through a series of one-way valves. This makes the calf the ‘second heart’ of the vascular specialist. It’s a no-brainer when you see it: the second heart only pumps when the body is moving. When standing still, stops pumping.
The calf pump ceases to work and blood backs up in the legs, straining the one-way valves. Repeat this for years and the valves weaken, leading to the symptoms of varicose veins and chronic venous insufficiency – the aching, the heaviness, the swelling by the end of the shift, the bulging veins. This is not a ‘side risk,’ this is a risk! One of the most common causes of varicose veins in the workplace is prolonged standing, and standing work increases the risk of hospitalization for varicose veins. The standing trades clearly over-represented with high rates of retail, nursing, teaching, hospitality, manufacturing.
Notice the pattern. The same culprit is responsible for the back-pain finding: the vein finding point is the same, the standing is the same, the stillness inside it itself is the same. The calf that never contracts is the same posture that makes a person a pain developer. One fix takes care of both.
Where shoes actually come into this — and where they don’t
Now the footwear question makes sense, because you can ask it precisely instead of vaguely. The honest answer: a shoe’s job here is narrow. It can make small, frequent weight-shifting easier and more comfortable, or it can fight it.
A shoe that lets your foot feel the ground and move encourages the micro-adjustments that protect you. A stiff, heavily structured shoe that locks the foot into one position discourages them — it makes staying still the path of least resistance, which is the exact thing you don’t want. That’s the legitimate, evidence-shaped case for a more flexible work shoe. Not “barefoot shoes cure back pain.” Just: the shoe should permit movement, not suppress it.
But a few claims floating around the minimalist-shoe world get ahead of the evidence, and on a health topic that matters:
- “Orthotics are a crutch that weakens your feet.” That’s marketing, not medical consensus. For diagnosed conditions — plantar fasciitis, certain arch problems, diabetic feet — orthotics are prescribed for good reason. If a podiatrist has you in them, a blog post is not the place to talk you out.
- “Switch to minimal/zero-drop shoes and your pain resolves.” Switching abruptly is how people hurt themselves. Feet conditioned to thick support for years need a long ramp. The shoe is a small lever on the movement problem, not a cure for it.
- “Good shoes fix brain fog and sleep.” No study supports a clean causal chain there. Less pain plausibly helps you feel better; that’s not the same as a footwear-to-sleep mechanism, and dressing it up as one is exactly the overreach that gets a health article flagged as junk.
If you want a shoe that helps, the one real criterion is whether it lets your foot keep moving through the shift. Flexibility and a roomy toe box serve that. A rigid sole works against it. That’s the whole footwear story, and it’s smaller than the shoe ads want it to be.
What to actually do tomorrow
The fix is mostly behavioral, and the shoe is a supporting actor:
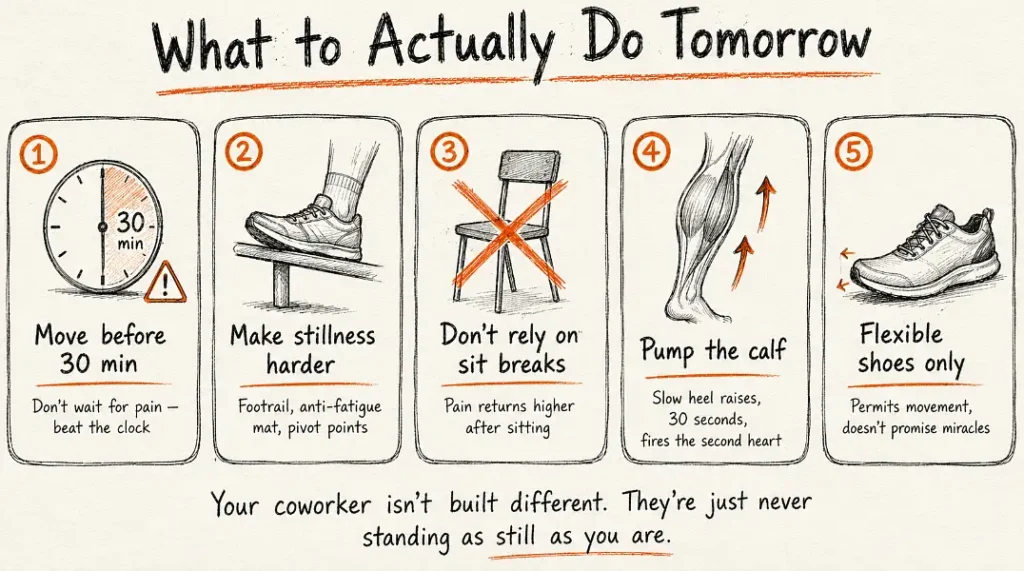
- Move before the 30-minute mark, not after. The pain has a head start measured in half-hours. Beat the clock — shift your weight, take three steps, change which foot carries you, before anything starts to ache. Waiting until you feel it means you’ve already lost the early window.
- Make stillness harder to fall into. A footrail to prop one foot on, an anti-fatigue mat, a reason to pivot — anything that nudges you to keep redistributing load. The non-pain developers do this without thinking; you may have to do it on purpose.
- Don’t count on the sit-down break to undo it. Useful, but it doesn’t reset the clock, and pain can come back higher afterward. Movement during standing beats recovery after it.
- Pump the calf on purpose. A few slow heel raises every so often fires the second heart and clears the pooled blood — thirty seconds, and it does more for your legs than standing flat for an hour. If swelling or aching legs are already a pattern, this matters as much as anything you put on your feet.
- Pick shoes that allow movement, not ones that promise miracles. Flexible sole, room for the toes, nothing that bolts your foot into a single position. Skip anything sold on curing fatigue, fog, or back pain outright.
Your coworker isn’t built different. They’re just never standing as still as you are — and now you know what they’re doing, you can do it on purpose.
This is general information, not medical advice. Persistent back, foot, or leg pain — or any diagnosed foot condition — is worth a conversation with a doctor or podiatrist before you change footwear or routine, since standing pain can overlap with issues that need real treatment.
Sources
- Coenen et al. (2017), systematic review of prolonged standing and musculoskeletal symptoms — dose-response thresholds (~71 min; ~42 min in pain developers). Gait & Posture / ScienceDirect.
- Threshold study on office workers, ~30-minute onset of low-back and foot pain in a 1-hour standing task. PMC8871560.
- Gallagher, Nelson-Wong & Callaghan (2011); “Early static standing is associated with prolonged-standing-induced low back pain” (2015) — pain developers vs. non-pain developers, movement frequency, ~44% PD rate. PubMed 21802955; 26340276.
- Systematic review/meta-analysis of standing pain developers, including the failed 15-minute seated break finding. Scientific Reports (2023); PMC10115839.
- NIOSH review, “Evidence of Health Risks Associated with Prolonged Standing at Work.” CDC.
- Calf muscle pump as venous return mechanism; prolonged standing as a risk factor for varicose veins and chronic venous insufficiency, and raised hospitalization risk. Banner Health; Mayo Clinic Health System; PMC7363262; PMC9299570.

{kind=link}